
What’s the Best Anti-Snoring Device? (Sleep-expert reviews top 13 criteria)
Estimated reading time: 16 minutes
The best anti-snoring device is only prescribed after you’ve been screened for Obstructive Sleep Apnoea / Apnea (OSA).
The best one:
Stops your snoring
Costs you the least money (because it isn’t a false economy)
Creates the least side-effects (and helps you sleep and breathe at the same time)
So, if you’re wondering what’s the best anti-snoring device, then read this independent (no advertisements or affiliate links!) sleep-industry expert review.
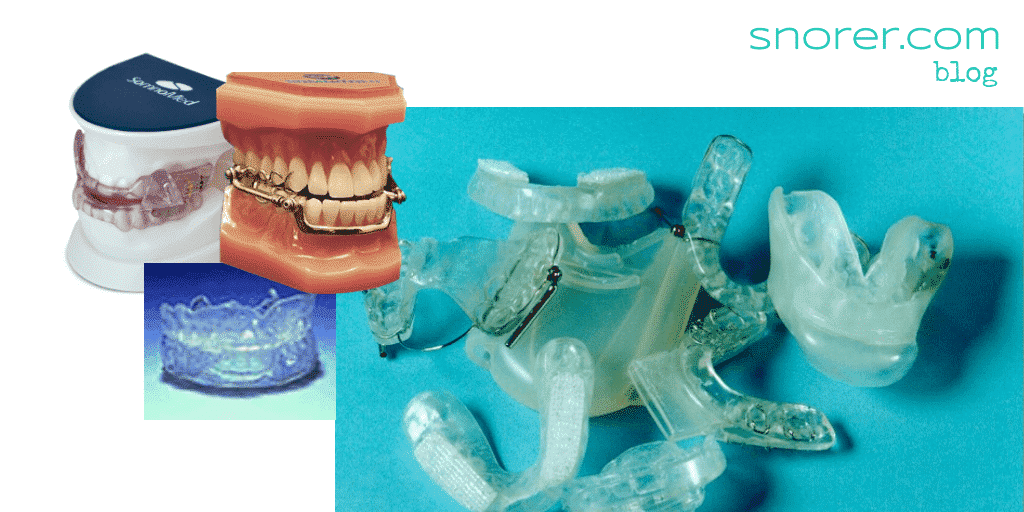
These devices, which in their simplest form loosely resemble an athlete’s mouth guard, help open your airway by bringing your lower jaw (mandible) and tongue forwards while you sleep.
This movement (known as ‘protrusion’) increases the space behind your tongue. While a dentist-made appliance may appear expensive, ‘cheaper’ do-it-yourself kits are available.
This independent, expert review examines the pros and cons of custom-made versus DIY anti-snoring devices.
If you have difficulty breathing through your nose, address this before you consider an oral appliance. Consult your GP if the issue persists.
While an oral appliance should not stop you breathing through your mouth, it will certainly present a restriction.
Nasal breathing is ideal. Read more about this in my post about snore-relief products available without prescription.
The latest NICE Guidelines (National Institute of Health and Care Excellence) for the United Kingdom, describe an anti-snoring device as below. Check out their interactive pathway for obstructive sleep apnoea.
A mandibular advancement splint is an oral device used to treat sleep-related breathing disorders. It is worn over the upper and lower teeth, and holds the lower jaw forward, thereby increasing space at the back of the mouth and decreasing snoring and sleep apnoea. A custom-made mandibular advancement splint is formed from a dental impression taken by a dentist, which is used to make the splint in a laboratory. It is then fitted by a suitably trained general dental practitioner. A semi-customised mandibular advancement splint is formed using a dental impression taken by the patient, which they send to the manufacturer to make the splint.

 ORCiD
ORCiD
Mandibular Advancement Device Webstory:

It’s just snoring – right?
Anti-snoring devices (Mandibular Advancement Devices – MADs) or ‘gumshields for snoring’ are big business on the internet and in some pharmacies, typically when self-help fails.
Despite the lack of prior sleep apnoea screening.
Indeed, the United Kingdom’s NHS website makes reference to MADs but fails to differentiate between custom-made and Over-the-Counter (OTC) snore-stoppers!

So, the challenge as a hasty snorer is:
How to choose one that actually works?!
Snoring aids and cures are increasingly popular as we recognise the impact poor sleep has upon our health, daytime functioning and work performance.
But what works?
A news article “Ten Snoring Cures” reviewed 10 ‘cures’ available in the UK.
The journalist tried to stop his own snoring, with chin straps, sprays, pillows and ‘gumshields’, aka anti-snoring devices.
He had little success and concluded his review by quoting a UK snoring expert, Consultant Respiratory Physician, Dr Tom McKay, from Edinburgh Royal Infirmary Sleep Centre, UK, as saying:
‘Sprays don’t have any great effect although nasal steroids have a small role if you’ve got nasal congestion. It can help to lose weight or avoid alcohol last thing at night or to sleep lying on your side. Various forms of gumshield are reasonably successful – maybe 50 or 60 per cent.’
So, its a reasonable question to ask….
Which Anti-Snoring Devices really work?
‘Gumshields for snoring’ could more accurately be described as mandibular advancement devices (MADs).
They are also known as intra-oral devices, mandibular repositioning devices (MRDs) or even sometimes mandibular advancement splints (MAS) !
But there are essentially just two categories:
Over-the-Counter (OTC) ‘gumshields’
Prescription, Custom-Made Dental Appliances
In this updated for 2023 review, I examine how both categories of anti-snoring device measure up against my Top 13 criteria for choice (see call out box) to determine which ones really work, and if they’re safe and effective.
And the best bit?
Each section concludes with my verdict and there’s a free bonus at the end!
L
Lucie Ash – Director Somnwell
 if you are looking for impartial advice about snoring from an expert in the field, the highly respected Adrian Zacher should be your go to. We applaud Adrian’s work, to raise awareness about the health implications of snoring, and the importance of prescription, custom made devices for long-term success
if you are looking for impartial advice about snoring from an expert in the field, the highly respected Adrian Zacher should be your go to. We applaud Adrian’s work, to raise awareness about the health implications of snoring, and the importance of prescription, custom made devices for long-term success
Top 13 criteria for choosing an anti-snoring device
Snoring may be a symptom of obstructive sleep apnoea/apnea (OSA).
Without first being screened for OSA your purchase of an OTC anti-snoring device, could harm you and if you snore because you have undiagnosed Obstructive Sleep Apnoea (OSA) the OTC gadget delays effective (and free on the NHS!) treatment that will prolong your healthy life.
Consult a sleep-trained pharmacist to learn how to stop your snoring.
The pharmacist will screen you for OSA and decide if you’re ‘just’ a snorer or if your snoring needs investigating.
Your GP may be able to help you – but they may not know much about sleep apnoea as sleep is not part of core medical training. We provide expert written GP Guidelines to help.
In the UK, you can also find sleep-trained dentists who can screen you and recognise Obstructive Sleep Apnoea/Apnea (OSA) symptoms2, make custom anti-snoring devices for snorers, without a prior medical diagnosis, or if they suspect OSA refer you on for further investigation.
Oral appliance therapy is considered a second-line option for OSA (which means that PAP is first-line [the first treatment option] and only after PAP failure would an oral appliance for OSA be considered).
Learn more about dental appliances for sleep apnoea.
No. 1. Clinical evidence (proof) that the Anti-Snoring Device works
Medical and dental experts review medical devices (clinical research) to establish if they work.
Their research produces data and information which can be thought of as ‘proof’ that something does or does not work, and how well it works in certain circumstances.
The evidence they create is also judged for quality.
Judging Anti-Snoring device (MAD) research quality
When selecting an anti-snoring device, it’s important to look at this clinical evidence.
To judge the quality of a mandibular advancement device’s (MAD’s) clinical research evidence, you need to look past the headlines claiming “Clinical research– tick”.
What was the outcome of the research?!
Typical patient-centred measures of outcome
Measurement of what patients perceive as important effects from wearing an MAD typically include:
- Partner reported snoring (derrr… a no-brainer!)
- Daytime sleepiness
- Quality of life
- Adherence (long-term use)
- Device preference
Gumshields or ‘Boil-and-Bite’ anti-snoring devices, have been clinically researched head-to-head against custom-made, prescription, adjustable anti-snoring devices and found to be lacking.
Our results suggest that the thermoplastic device cannot be recommended as a therapeutic option nor can it be used as a screening tool to find good candidates for mandibular advancement therapy.3
…patients overwhelmingly found the ready-made MRD difficult to tolerate…4
…96% of patients reported minor adverse events, which related predominantly to discomfort.4 [referring to a study by Dr. Tim Quinnell 5
Today, clinical research has established that custom made MADs are first-line therapy (the default first option) for snoring and mild obstructive sleep apnoea / apnea.
MAD research now focuses on:
Predictors of satisfactory outcome before purchase (who will benefit and why) and which type of custom made MAD is most effective for a given genotype (which MAD is best for YOU as opposed to a vanilla approach).
It is not enough to say that an MAD has been clinically researched. Such research may have proved the MAD didn’t work!
A positive outcome from clinical research can be thought of as a ‘guarantee’ of sorts.
My advice is to do your homework (grab the Bonus Mouthpiece Guide at the end) and be guided by a sleep-trained dentist. You can find one via our Links page.
[Note: Below is an advanced topic about typical MAD research metrics. So, if you’re new to clinical evidence, feel free to skip this tip].
- Total sample size (the ‘N’ or number of patients who used the device)
- Could they tolerate it in their mouth (known as tolerance)
- How many hours they used it for each night (known as compliance)
- How many nights they used it for per week (part of the compliance metric)
- Partner reporting of cessation of snoring
- Perceived sleepiness before and after use
- Before and during use blood oxygenation level
- Before and during use AHI (apnoea hypopnea index – an index used to indicate the severity of sleep apnea. The number of apnea and hypopnea events per hour of sleep)
- Whether a placebo was used with a control group
- Whether patients crossed over to a different therapy / device
- Whether the researchers and/or patients were ‘blind’ (who was aware which device was a placebo or an actual MAD?)
- Has the research been published in a high profile and peer-reviewed journal? (This means other experts in the field judge it for quality)
No. 2. Anti-Snoring Device costs
OTC gumshields and ‘treatments’ might appear cheaper than custom-made, prescription appliances & dentist fees, BUT…
Are they a false economy?
Why use a dentist to get an Anti-Snoring Device (MAD)?
Financially, its tempting to cut out the dentist.
After all, a large part of the cost to you when purchasing a mandibular advancement device, is their clinical time.
The device fees vary, but what are you paying for?
That is what they do.
While Dentistry may initially seem expensive, the risks of not using an expert are considerable.
Remember, you are relying on the anti-snoring device to hold open your airway while you sleep. Think carefully before you choose.
Some dentists are specially trained in snoring and sleep apnoea / apnea, known as sleep-related breathing disorders (SRBD) and work closely with medics.
Dentists with a special interest in sleep, can help you find the correct balance of benefits versus side-effects.
If you have certain medical conditions, or grind your teeth, you might break an OTC ‘gumshield’ whilst you’re asleep. When you are asleep you cannot spit out pieces of a broken gadget. You could INHALE or SWALLOW pieces.
You can find sleep-trained dentists on our Links page. In the UK, look for the British Society of Dental Sleep Medicine.
Don’t do it.
The terrifying thought of bits of MAD breaking off and being inhaled while you sleep, should surely make you realise you need to see a sleep-trained dentist and use a prescribed custom-made, adjustable anti-snoring appliance, made to quality standards.
In case you’re wondering, I’m not a dentist.


Tired of the sleepiness and the snoring?
Then read our free, definitive step-by-step how to stop snoring Guide.
No. 3. Comfort and bulk of Anti-Snoring Devices (MAD)
An MAD that is so uncomfortable to wear, soon ends up being thrown across the bedroom or just left in the bathroom at bedtime…
Both the design and clinical expertise in how an anti-snoring device is supplied, directly impacts your likelihood of successfully wearing it (and therefore whether it stops your snoring) – particularly during the first two weeks of use.
This is when most people who aren’t going to get on with them, quit. It might seem obvious:
but if you don’t wear it – it doesn’t work.
Generally OTC gumshields for snoring are “one-size-fits-all”. They have to be bulkier in size to adapt to your teeth than custom-made devices.
This would mean it feels like you are squeezing a tennis ball into your mouth – Oh, and then you’re expected to sleep!
A sleep-trained dentist will ensure that your MAD fits properly and doesn’t hurt.
They will also ensure you know how to put the device into your mouth and get it out again.
As a general rule, custom-made anti-snoring devices are less bulky than ‘gumshields’.
Due to the lack of accuracy of the ‘fit’ and one-size-fits-all approach of gumshields, they may be too large, too small or take up so much room in your mouth you can’t close your lips and you find yourself dribbling attractively!

No. 4. Will an Anti-Snoring Device (MAD) damage my teeth and gums?
You wear these things in your mouth.
What impact will it have?
Its quite possible that a gumshield will place excessive load upon an individual tooth/teeth.
Over time your teeth will move. It will hurt.
And you will either:
- stop wearing the mandibular advancement device and accept the financial loss (good luck trying to get a refund on a used product), or…
- under duress from your partner and family, continue wearing it and risk losing the tooth or an expensive crown/cap/bridge.
Prescription Mandibular Advancement Devices on the other hand, can be designed to avoid certain teeth if they are identified as at risk.
An expert sleep-trained dentist can help identify (and save that tooth) if it could not withstand the lateral loading required.
A dental technician would ‘block out’ the identified tooth and not include it in the custom-made device.
All anti-snoring devices will aggravate your oral hygiene.
However, a sleep-trained dentist would ensure BEFORE you had an MAD, that your hygiene and oral condition (teeth, gums and jaw-joints) were satisfactory before you began to use it.
Try to keep the device as clean as possible. Use your toothbrush and toothpaste on it each morning. Don’t use chlorine based denture cleaners on gumshield based devices – it makes them hard and brittle (unusable) rapidly. Instead, use a baby bottle sterilising fluid (follow the manufacturer’s instructions).
Brush and floss your teeth carefully and consider using a chlorhexidine mouthwash. If you spit blood when you clean your teeth consult a dentist/hygienist.
‘Boil-and-Bite’ devices will flex when worn and over time, this will procline (tilt forwards) your lower incisors and retrocline (tilt backwards) your upper incisors.
Certain custom-made anti-snoring devices are designed to avoid this tooth tilting movements.
Consult your sleep-trained dentist.
No. 5. Will an Anti-Snoring Device damage my jaw-joints?
Jaw pain is truly horrible and once you have a jaw pain problem it persists.
All types of mandibular advancement device (MAD) work by moving your lower jaw forwards, and the amount it does this to be effective, and not hurt too much, is specific to you.
Some gumshields for snoring are only adjustable in large increments, while others you have to fit the device – rather than the device actually fit you (again you may lose your money).
Custom made, adjustable, prescription MADs really win when considering your jaw joint. In fact, it’s possible, with some of the custom made ones to start off wearing it with no (or very little) change in your jaw position.
While of course it won’t initially prevent snoring in this position, the dentist will gradually advance your jaw until you stop snoring over a matter of weeks or perhaps even longer (this is known as titration). This gives you, your device (and your jaw joint) time to get accustomed.
Which means you STOP SNORING!
And don’t permanently harm yourself. Yay!
Your sleep-trained dentist will screen you for sleep apnoea, assess your teeth, gums and examine your jaw joints.
They will take X-rays and put things right beforehand if necessary. If it doesn’t look like its a good idea, they’ll suggest:
- You DON’T have one,
- Explain why,
- And direct you to appropriate help.
If everything is OK, they’ll monitor the effect the MAD is having upon your teeth, gums, jaw joint and snoring.
If your jaw joint isn’t healthy before you start using an anti-snoring device then it may cause irreversible harm. (The exception is when a specialist sleep and jaw joint pain [Temporo-Mandibular Joint Dysfunction or TMD] dentist prescribes a device for BOTH issues.)
A sleep-trained dentist would know what to avoid and ensure you did not experience premature posterior contact (see call out box) that would damage your jaw-joint.
Premature posterior contact
This gets a bit technical.
A common problem particular to ‘gumshields’ occurs when the device is adjusted forwards known as ‘protrusion’ (you might do this in an attempt to increase the effect – and stop the snoring noise). The upper and lower parts of the device may then come into contact on just your back teeth.
This acts like a ‘bit’ for a horse – it gives you something to chew on. It ‘gags’ open the bite (keeps your jaws more open than they should be) and this uneven bite places enormous load on your jaw joints.
It would be even worse for your jaw joint, if this was on one side only, and as you close your mouth, your jaw has to ‘rotate’ around this ‘premature contact’.
What the above means, is that your jaw has to move in unnatural ways.
This hurts.
And if you use the device in this position (because you’re trying to appease your partner) you may irreversibly damage your jaw joints.
No. 6. Retention / Fit of your Anti-Snoring Device (MAD)
How well your anti-snoring device fits, is known in dental terminology as ‘retention’.
But retention has two meanings in Dental Sleep Medicine (DSM is the term for MADs used to help with sleep-related breathing disorders, including snoring and OSA).
The first meaning is how well it keeps ‘hold’ of your teeth, or to put it another way, how well it ‘clips on’ or stays in place.
Most MAD designs rely upon its ability to ‘clip’ into place to then be able to hold your jaw forwards – and stop you snoring.
The second DSM interpretation of ‘retention’ relates to the MAD’s ability to hold open your airway, retain your jaw in a forward position, and prevent you from snoring.
So, the right amount of retention (or fit) is essential for it to work.
Over-the-Counter ‘gumshield’ vendors make their money by relying on you being too lazy to seek a refund when it doesn’t work.
This is unavoidably technical. So, feel free to skip to my verdict.
Due to the necessary choice of thermo-plastic (it softens and becomes adaptable to you, when heated in boiling water) material used in ‘boil and bite’ devices, getting and keeping the right degree of retention, for the long-term is nigh on impossible.
The material ‘wants’ to go back to its original shape as it cools down, which is technically due to both the elastic memory and elastic recovery of the material. There’s more about the material used in the Lifespan or ‘Cost per wear’ section below.
Custom-made dental devices for snoring are made for you (on prescription) from raw materials by a registered dental technician. While the materials used vary, they usually only become thermoplastic (soften when warmed up) when heated over 100 deg C.
On the other hand, ‘Customised fit‘ devices are the ‘Boil-and-Bite’ gumshield type of MAD (and I know you know water boils at 100 deg. C!).
Boil-and-Bite gumshields for snoring as a general rule, cannot provide good retention of your teeth.
Without good retention or ‘clip’ to your teeth, gumshields will not stop you snoring.
End.
No. 7. Can I adjust the position of my Anti-Snoring Device (MAD)?
The ability to adjust the forward position of your jaw (adjust the protrusion to prevent snoring) impacts upon both comfort and how well it works.
The optimum position is unique to you. It has to be just far enough forward to prevent you from snoring, yet not so far forward, it hurts your jaw joints.
Fixed devices (sometimes called ‘monobloc’ devices) take an arbitrary approach to the forward position of your lower jaw (they guess).
This primitive design (exhibited by both over-the-counter gumshields and some old tech custom-made ones) is likely to be less than ideal for comfort and of course effect.
Which leads neatly in to how anti-snoring devices work:
How do anti-snoring devices work?
In a word: protrusion.
In the short video clip below, I explain how ‘protrusion’ (holding the jaw forward) opens the space behind your tongue (and what to avoid when choosing an anti-snoring device).
Click the video bottom-right to view the sound controls slider.
For the MAD to prevent snoring it must prevent your mouth from falling open.
You should NOT need a chinstrap in addition to your anti-snoring device. If a chin straps is suggested then:
You need a different MAD.
If you’re trying to ensure you breathe through your nose and stop your mouth falling open, then read Chinstraps for snoring? Safe, Effective or Dangerous? [new window]. In my chin strap review, I examine if they have a role for snoring and obstructive sleep apnea (OSA).
If you can only breathe through your mouth and/or sometimes struggle to breathe through your nose, then consult your GP and seek an ENT assessment.
Custom-made, adjustable MADs are inherently adjustable (the clues in the name!)
The important thing to understand about adjustable MADs relates to their range of movement, and:
- Whether this is sufficient
- Whether it dictates a hard to tolerate initial position
The most modern custom-made adjustable MADs have between 8-10mm range of movement. If more is needed – you will most likely need a remake (more money).
Clearly, fixed or monobloc devices fail this test 🙂 A new anti-snoring device would need to be made if the jaw position was incorrect. Adjustable anti-snoring devices need to have sufficient range of motion to coincide with your jaw range of motion – or you must start in a forward jaw position, which may impact upon your ability to get along with the MAD initially.
No. 8. Life-span or ‘cost-per-wear’ of your Anti-Snoring Device
To ensure your purchase of an anti-snoring device (MAD) is not a waste of money or a false-economy, you have to consider:
- Its outright price (don’t forget the clinical fees) and VAT (if its for snoring)
- Its length of useful life
Amongst other things…
A material that softens in boiling water called ‘Ethylene Vinyl Acetate (EVA) or EVA’ is commonly used in gumshield type anti-snoring devices.
- This material absorbs saliva from your mouth (and also any cleaning chemicals that may then leak back out into your mouth overnight – nice).
- They are damaged if you grind your teeth because the material is soft and elastic.
- Their typical lifespan is 6 months to 1.5 years before the EVA constructed gumshield becomes too smelly and unpleasant to use.
- They also distort and place high lateral loads on your front teeth – making them very sore in the morning.
Some early design variants of custom-made anti-snoring devices, are also made from EVA ‘blow down’ or vacuum formed blanks of CE marked material by a registered dental technician.
However, most are typically made from a type of denture acrylic (polymethylmethacrylate) or ‘PMMA’, and as such are stronger and less likely to absorb saliva than EVA materials. Some new variants are made from a type of ‘Nylon’ (polyamide) and are very strong in thin section (see Comfort and bulk above). This means they will last longer and therefore the ‘cost per wear’ may be reduced.
In the UK, it is also possible to obtain a custom-made anti-snoring device manufactured entirely from metal (known as ‘Chrome’ = Cobalt chrome wiki link: http://en.wikipedia.org/wiki/Cobalt-chrome ![]() ) While this type of manufacture may cost more (they are more time consuming to make) the material cross-section is extremely thin (fractions of a millimetre are possible) making the bulk in your mouth minimal (see comfort and bulk above). Additionally, the metal device does not absorb saliva or cleaning agents.
) While this type of manufacture may cost more (they are more time consuming to make) the material cross-section is extremely thin (fractions of a millimetre are possible) making the bulk in your mouth minimal (see comfort and bulk above). Additionally, the metal device does not absorb saliva or cleaning agents.
The downside is that any adjustment of ‘fit’ of metal devices may be problematic and over time the clasps (bits that wrap around your teeth to hold [retain – remember that?] the device in your mouth) may ‘relax’ and need adjusting.
Broadly speaking its a sliding scale of cost versus lifespan.
The high-end devices using nylon or chrome are thinner and less bulky but are also difficult (if not impossible) to adjust. This does not mean to say its a problem, they just have to be perfectly made.
So, if its not – then it needs to be remade: Do not accept a poor fitting custom made anti-snoring device.
No. 9. Control of mouth opening (Does the MAD do it?)
When using a mandibular advancement device (MAD) it is essential that your mouth does not fall open for effective snoring relief, which if permitted would make your airway narrower than it would be without a mandibular advancement device!
It should not be necessary to resort to a chin strap to control this. Yes, I’ve been over this point in point 7 Can I adjust the position of my anti snoring device above, but…
Why does vertical opening matter?
The lower jaw rotates backwards as it opens which further narrows your airway and makes snoring worse (or if you have sleep apnoea / apnea may increase the severity and duration of apnoeaic episodes).
If your jaw is protruded with a mandibular advancement device (MAD) and your jaw falls open your airway may be narrower than without using an MAD.
See the three X-ray diagrams below, to understand why vertical opening with an MAD should be avoided.
The red dots highlight how the airway increases / decreases with protrusion and vertical opening.
Images courtesy of Dr Ulrich Huebers DDS.
The diagram (below left) shows the size of the airway in your throat without a mandibular advancement device (MAD).
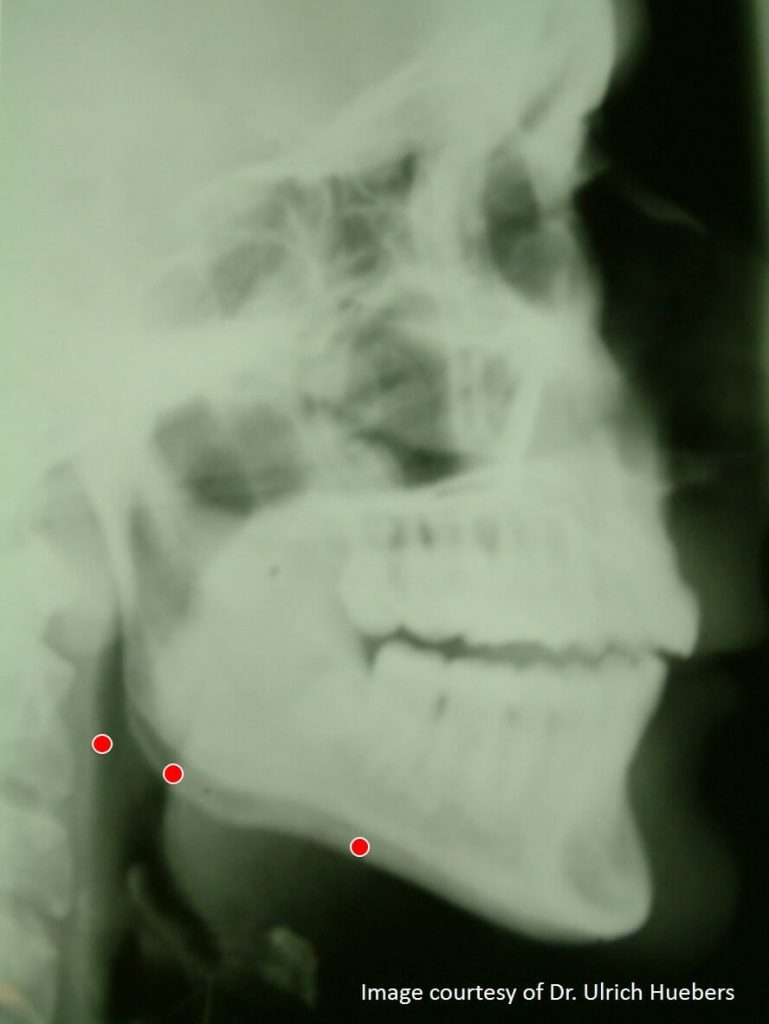
The diagram (below centre) shows the ideal situation. The mandibular advancement device advances the jaw and opens the airway in your throat.
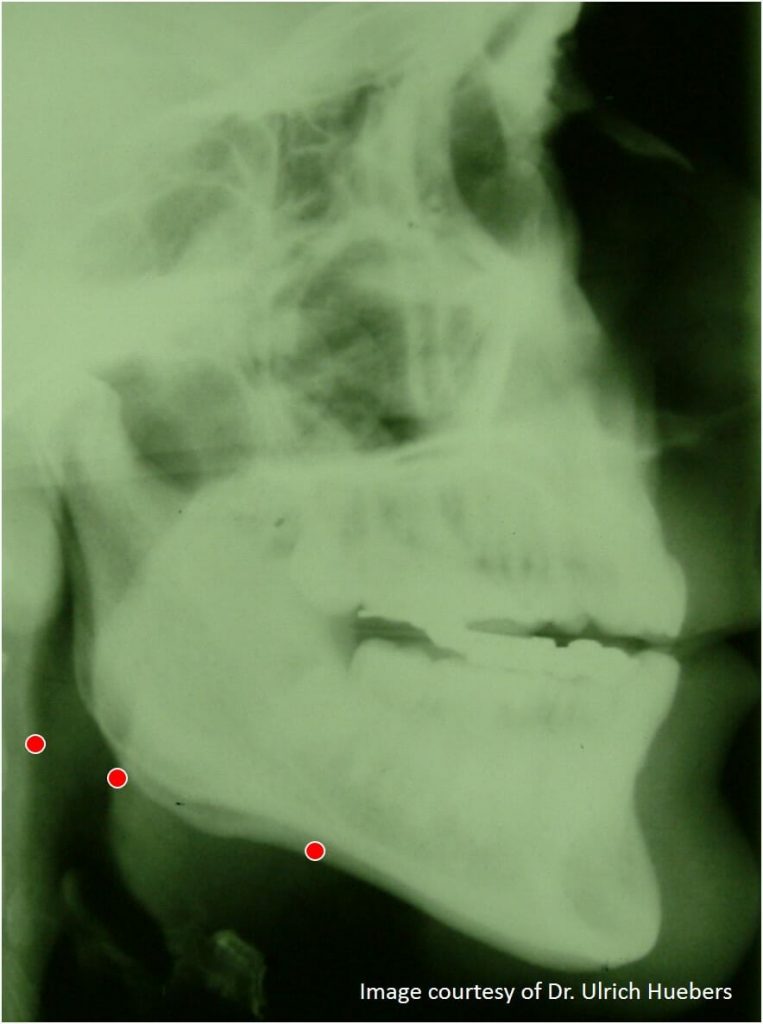
The third diagram (below right) shows how the airway becomes narrower with both protrusion and vertical opening. Disaster.
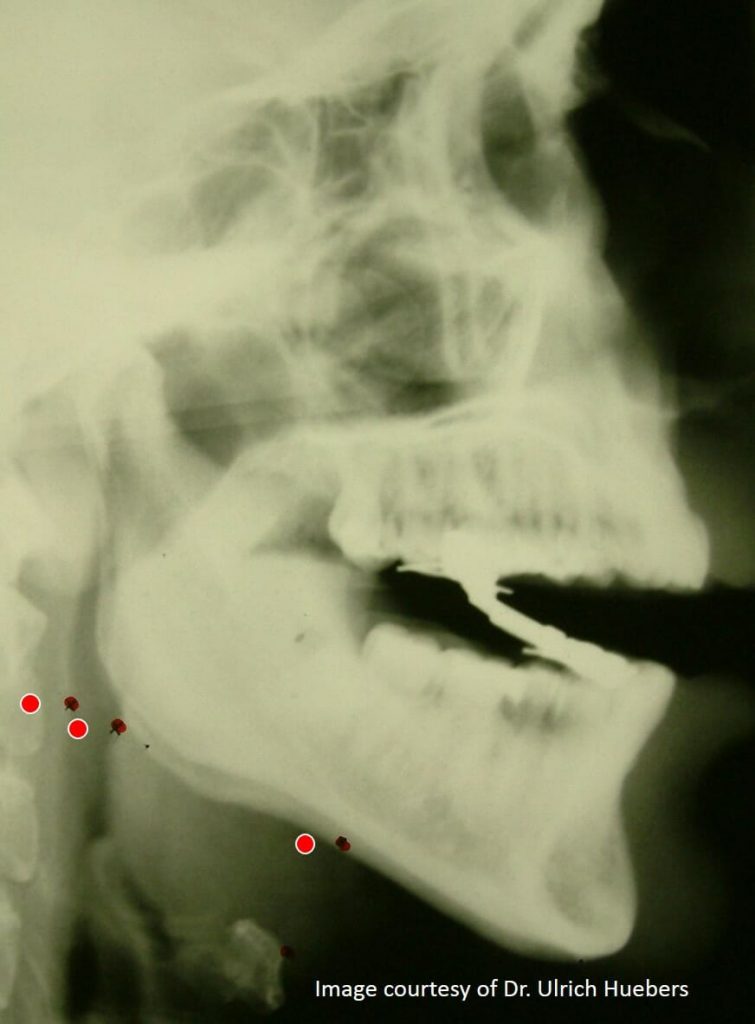
Both categories of MAD (Boil-and-Bite gumshield and custom-made MADs) can fail when examined against this important test metric.
- Jaw advancement must increase as the mouth opens (protrusion must increase proportionally [to maintain the same effect] if vertical opening occurs).
- Less protrusion correlates with:
- Less side-effects (including less risk of tooth movement and jaw pain)
- Increased tolerance and improved long-term compliance.
An interincisal opening (the distance measured between the upper and lower front teeth) of more than 5 mm has been associated with lower patient adherence (long-term use), perhaps as a result of discomfort.6
Minimal vertical opening (as in just sufficient to permit the lower jaw to advance without the upper and lower teeth hitting each other) should routinely be considered ideal. More than this may be necessary in selected cases where:
- the tongue is large
- the jaw is small
However, opening beyond 5mm (measured between the incisors) is uncomfortable, inhibits lip closure and detrimentally impacts long-term use. A design principle for MADs is control of vertical opening (note my previous comment about not needing a chin strap).
Finally, consider your sleep position. Avoid sleeping on your back and ensure that your neck is inline with your body. Choose a supportive pillow. Learn more about positional therapy and anti-snore pillows.
No. 10. Ability to move side-to-side (lateral movement)
It might seem obvious, but unless the MAD is worn, it cannot stop your snoring.
As such, it must be comfortable to use. Part of this comfort equation is the MAD not creating a ‘trapped’ sensation.
This may occur when the lower jaw is unable to move from side-to-side.
Some MADs (both custom-made and ‘Boil-and-Bite’) exhibit the capability to move laterally (side to side) while some do not. My viewpoint is that you should look for one that does permit movement.
If you grind your teeth (brux) then this will significantly impact the life-expectancy of your MAD. In fact, you may work harden metal components necessitating their earlier replacement, than would otherwise be expected.
Finally, while it is perhaps a contentious area, if you routinely ‘brux’, then an anti-snoring device that does not permit side-to-side (lateral) movement may actually disrupt your sleep. One theory suggests that this is because your attempts to move are hindered.
The opposing theory suggests you will no longer brux when your apnea is resolved. The jury is out.
No. 11. Does the Anti-Snoring Device mechanism invade your tongue-space?
Ever had a filling or a crown? You may recall how you were very conscious of it.
You probably explored it with your tongue and it felt alien. Every anti-snoring device will feel huge in your mouth when you start to use it.
Consequently, less is more!
Less physical presence in your mouth, squashing your tongue, enhances your ability to initially accept it and keep using it – and stop snoring…
The concept behind an MAD is to advance the jaw, and in turn, move the tongue forwards and away from the back of your throat.
This increases your airway dimensions and improves tissue tone, which stops you snoring.
So, when an MAD is too bulky, it squashes your tongue. Which is self-defeating.
Typically, gumshields are bulky and squash your tongue. They may even have rough or sharp edges which may cause tongue ulcers.
Technically, this may occur with ‘gumshields’ at the junction between two materials, typically with devices that have a hard-outer shell and a softer thermoplastic liner, or when they are crudely ‘adjusted’ with home equipment i.e. scissors!
Construction
Some primitive custom MADs are bulky and invade tongue space. Materials technology is continually improving, and thinner cross-section devices are now appearing on the market using laser sintered polyamide (a type of nylon).
While traditionally manufactured metal (known as ‘chrome’) devices are available. These may be expensive to make (as they are labour intensive) and may necessitate plastic and metal combined devices, which builds in failure points (because dissimilar materials exhibit different mechanical properties).
Placement of the adjustment mechanism
The placement of adjustment mechanisms in the tongue space is uncomfortable and counter-productive (see concept note above in introduction to this point). Some early custom MADs used orthodontic screw mechanisms in the palate or inside the lower jaw (lingually).
A sleep-trained dentist will guide you when you choose. To get informed for that conversation download our free, evidence-based How to Choose a Mouthpiece Guide.
If you can’t wear your MAD, then it’s pointless having it. Consequently, comfort has to be a pivotal deciding factor when selecting one.
Anything placed where your tongue can contact it, is a negative. Remember less is more, when it comes to MAD design.
No. 12. Easy to Keep Clean (Extend useful life, hygiene)
Consult your dentist and the MAD manufacturer’s instructions on how to clean your MAD.
I would suggest that broadly speaking you should (every time you remove it in the morning) use a toothbrush and toothpaste on the device before/after cleaning your teeth.
Floss if you have the enthusiasm and discipline… and consider using a chlorhexidine mouthwash too.
Having worked in this industry for longer than I care to remember, I know that MADs must be:
- Easy to keep clean
- Not absorb cleaning fluid or saliva
- Ideally not have intricate mechanisms to retain food and bacteria
- Be entirely made of one material
Bacterial biofilm (a slimy film of infectious microbes) will form on the device.
It’s important to pay extra attention to your oral hygiene (and keep the MAD clean with a toothbrush immediately you remove it in the morning).
These materials absorb saliva (and cleaning fluids) so bacteria are drawn into the material itself – not just on the surface. Ewww.
The use of materials with better properties, more suited to long-term use in your mouth, should have less detrimental impact. You will of course need to keep them clean and remove the biofilm – and keep your teeth and gums really clean.
See a dental hygienist if you need assistance keeping on top of this. Its an investment.
Prescription, custom-made MADs utilise materials that are better-suited to long-term use. They are inherently easier to clean and keep clean. This is vital when you consider the number of people who have gum disease (gingivitis) whose condition would be aggravated by an MAD, perhaps to such an extent that they risked losing a tooth.
Top Tip
If you are lucky enough to have a marble bathroom, make sure that the MAD cleaning fluid does NOT splash out (powder or granule type cleaning products are commonly a type of acid that permanently damages marble). Ideally, clean your MAD elsewhere! (Voice of experience! Customer reported the above to me when I ran Zacher Sleep Appliances).
No. 13. Side-effects of Anti-Snoring Devices (Mandibular Advancement Devices)
There’s always a down-side!
Or in ‘English’:
“You don’t get nowt for nowt”
The most common initial side-effect from using anti-snoring devices is related to saliva.
Some people find they dribble while wearing the device during the first few weeks of use (use a towel on the pillow).
Others may find they have a dry mouth.
This is normally transient and may arise during the ‘titration’ period (where the device is adjusted to gradually advance your lower jaw and stop you snoring).
If this occurs, the correct advice is to speak with your dental clinician. It normally resolves itself but do not suffer in silence.
This is due to the weight of your lower jaw (think gravity) and the muscles attached to it combining to attempt return of your jaw to its normal position. These forces are all transferred to your teeth and their roots.
This is why even the most wonderful anti-snoring devices are NOT suitable for children – because they would act like an orthodontic device and move their teeth in uncontrolled ways (exceptionally an orthodontist may prescribe an anti-snoring device for certain children with particular needs).
It is really important to keep things in perspective: Not snoring, breathing and sleeping at the same time or perhaps minor tooth movement?
However, as I have highlighted throughout this review all anti-snoring devices have side-effects.
A sleep-trained dentist would screen you for sleep apnoea, help you stop snoring and minimise (and if necessary correct) any side-effects. They also carry professional indemnity insurance and use prescription anti-snoring devices made to quality standards by registered dental technicians.

MY ADVICE
If you snore and self-help isn’t cutting it then don’t self-diagnose.
Instead, consult a sleep-trained pharmacist.
These accessible and underutilised healthcare professionals can actually help you!
FREE BONUS
Download our free, evidence-based, expert-written and jargon-decoded Guide (that’s a mouthful!):
> How to Choose a ‘Mouthpiece’ to Stop Snoring
You’ll learn about your options and be able to make more informed choices.
No registration is required.
All our Guides, including our award-winning snoring and sleep apnoea overview guide are free.
If you prefer you can grab the guides on Amazon (who sometimes insist on a minimum 99p fee) or free on Google Play Books.
Summary
This review has examined the best anti-snoring devices, both Over-the-Counter and custom-made, against my top 13 criteria, to help you choose an anti-snoring device that works, and is safe and effective.
My final verdict is that while a ‘boil-and-bite’ gumshield may prevent snoring for a short while (if you fit the gadget) they are ultimately a false economy and won’t work for long (if at all).
Longer-term, if you were to persevere with a ‘gumshield’ for snoring, it would:
- Create unpleasant and sometimes permanent, unmanaged dental side-effects
- Potentially irreversibly damage your jaw-joints
- And it delays potential OSA diagnosis and effective treatment
In conclusion, clinical research3 has established that ‘boil-and-bite’ gumshields are not valid as either a trial or treatment device.
Reading our Definitive Guide to OTC Anti-Snoring Device Manufacturers’ (ridiculous) claims.
The real question
The real question is:
Why do you snore?
My advice is to:
- Consult a sleep-trained pharmacist
- Get screened for sleep apnoea before you dive into any treatment and learn why you snore.
And then you will know exactly how to stop.
More Expert Reviews and “How-to’s” about snoring and sleep apnoea:
New products and methods to ‘cure the snore’ hit the market quite frequently. So while, personally I hate instant snoring cures, because I consider the balance of benefit-to-risk is generally against you, I have created more independent expert reviews for you to peruse.
Learn more about snore-relief products available without prescription, anti-snore pillows and my review of a novel positional therapy device designed to make you turn over.
For exclusive content subscribe to my newsletter:
Read this article on Linkedin or Medium.
Glossary
Anti-Snoring Device – generally considered a product worn in your mouth to stop you snoring.
Boil-and-Bite – a type of gumshield for snoring that may be adapted to you by softening the material in boiling water. See OTC below.
Custom-made – a bespoke device made exclusively for you by a registered dental technician, working to prescription, using CE marked materials. In Europe working to the Medical Devices Directive ![]() administered in the UK by the Medicines and Healthcare Products Regulatory Authority (MHRA).
administered in the UK by the Medicines and Healthcare Products Regulatory Authority (MHRA).![]()
DSM Dental Sleep Medicine – the management of sleep-related breathing disorders using dental devices.
Gumshield for snoring – see ‘Boil-and-Bite’ above.
Information Standard – NHS England’s Information Standard. Organisations that join The Information Standard are showing their commitment to producing good quality, evidence-based health and care information.
MAD Mandibular Advancement Device – Jaw advancing device, worn at night while asleep to hold forward the lower jaw to stop snoring and prevent obstructive sleep apnoea / apnea.
MAS Mandibular Advancement Splint – See ‘MAD’.
MRD Mandibular Repositioning Device – See ‘MAD’.
OSA Obstructive Sleep Apnoea – (also spelt apnea) When an individual is unable to sleep and breathe at the same time. Visually, a repetitive pattern of breathing interruptions (apnoeas) occurring while the individual sleeps, due to a physical obstruction in the airway.
OTC – Over-the-Counter product sold over the pharmacy counter or on-line without prescription, medical or dental assessment and without a review of medical/dental history.
Signposting – Is the medical term for directing people to the most appropriate professional to help them based upon their answers to some high-level questions.
Sleep-trained Dentist – A dentist that has undergone special interest training in sleep. As such they are able to obtain professional indemnity insurance.
Sleep-trained Pharmacist – A pharmacist that has undergone special interest training in sleep-related breathing disorders. Pharmacists are the most accessible and underutilised healthcare professional.
TMD – Temporo-Mandibular Joint Dysfunction. Jaw-ache or pain, due to abnormal or impaired movement.
References
- Snoring cures success ‘exaggerated’ http://news.bbc.co.uk/2/hi/health/1701735.stm [accessed 16th Oct 2016]
- Stradling, J. and Dookun, R. 2009, Snoring and the role of the GDP: British Society of Dental Sleep Medicine (BSDSM) pre-treatment screening protocol, British Dental Journal, 206, 307 – 312. Available here: http://www.nature.com/bdj/journal/v206/n6/abs/sj.bdj.2009.214.html [accessed 12 April 2017]
- Vanderveken OM, Devolder A, Marklund M, et al, 2008. Comparison of a custom-made and a thermoplastic oral appliance for the treatment of mild sleep apnea. Am J Respir Crit Care Med; 178: 197–202. Available here: http://www.atsjournals.org/doi/abs/10.1164/rccm.200701-114OC#.V9ukcFT_rio [accessed 12 April 2017]
- Ready-Made Versus Custom-Made Mandibular Repositioning Devices in Sleep Apnea: A Randomized Clinical Trial, Johal A, Haria P, Manek S, Joury E, Riha R. Ready-Made Versus Custom-Made Mandibular Repositioning Devices in Sleep Apnea: A Randomized Clinical Trial. Journal of Clinical Sleep Medicine : JCSM : Official Publication of the American Academy of Sleep Medicine. 2017;13(2):175-182. doi:10.5664/jcsm.6440. Available here: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5263072/ [accessed 18th June 2018]
- A crossover randomised controlled trial of oral mandibular advancement devices for obstructive sleep apnoea-hypopnoea (TOMADO). Quinnell TG, Bennett M, Jordan J, Clutterbuck-James AL, Davies MG, Smith IE, Oscroft N, Pittman MA, Cameron M, Chadwick R, Morrell MJ, Glover MJ, Fox-Rushby JA, Sharples LD. Thorax. 2014 Oct; 69(10):938-45. Available here: http://thorax.bmj.com/content/68/Suppl_3/A4.1 [accessed 18th June 2018]
- Pitsis AJ, Darendeliler MA, Gotsopoulos H, et al: Effect of vertical dimension on efficacy of oral appliance therapy in obstructive sleep apnea. Am J Respir Crit Care Med 166:860, 2002. Available here: https://www.ncbi.nlm.nih.gov/pubmed/12231498 [accessed 18th June 2018]
Created by Adrian Zacher



Thanks for writing such a great information and and sharing a great knowledge with newbies and patients like us.
Emily you are most welcome. Thanks for commenting.
Good article and helpful information. Nice to find out that the dentist is the specialist to go to (my general and ENT doctors couldn’t help). Thank you.
I do wonder about the affordability of a custom made MAD (device and visits to the dentist), and assume it will be a four digits affair…
Hi Dulce. Thanks for your comment and praise. I’m glad it helped you understand more about the role of the sleep-trained dentist.
Of course, I don’t know your currency – so if you’re in the UK I think you may be able to get a custom-made MRD and dental fees under 1000 GBP (proximity to London is the main variable here).
Hi Adrian,
A well-written, thorough coverage of the solutions out there.
Sharon Turnoy
Thank you Sharon. Kind of you to comment!
The real question should be as to WHY is there no mention of TSD’s! They can be the healthiest and certainly the cheapest dental solution for a snorer (even with mild apnea diagnosis) AND they DO NO HARM to try! I suspect BIG PHARMA figures in this assessment somewhere.
Hi Liza. Thanks for commenting. You are correct in that I made no mention of tongue retaining/stabilising devices (TRD/TSD) and I shall consider updating this article to rectify that omission. I would agree that custom-made, prescription TRD/TSDs may have a limited role when the patient has no teeth or there are jaw joint issues. However, they may be poorly tolerated and there is essentially less clinical evidence (compared to mandibular advancement devices) to support their role. See https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3899326/#B11
I would disagree wholeheartedly with your assertion that ‘they do no harm to try‘. Self-diagnosis of ‘snoring’ and then ‘treating’ yourself with anything is not very clever. Snoring may be a symptom of sleep apnoea and untreated sleep apnoea is a cause of considerable morbidity, reduction in quality of life, increase in healthcare utilisation and a cause of premature death.
As to the involvement of, as you put it ‘big pharma’, my bank balance says otherwise! More seriously, there are no sponsors, advertisers or ‘powered by’ behind Snorer.com or myself. I have no interests to declare.
This is a great article, well written and genuinely helpful amid a sea of supposed independent articles elsewhere on the web that are, in fact, merely a route to the sale of a product or service. Snoring is a tough gig for those who suffer from it (and beside it). You take the subject very seriously, you know what you’re talking about and you present a cogent, informed view to help sufferers make the right decisions for them. I’m a CPAP user and as effective as it is, going to bed looking like a Spitfire pilot every night is not great, and something that I’ve never quite got used to, so I’m always looking for cheaper, simpler, and let’s face it, more attractive, solutions for my sleep apnea. This is a great site from which to begin – and possibly end – your research into a better life as a sufferer. Thank you.
Paul. Thank you, for your kind words. I wish you every success in your quest. Here to help you.